Topic inspired by Dr. Eliott Lee’s (EM-3) ECG of the Block, October 21st 2015.
 At the end of the day: How do I know if my patient with a left bundle branch block (LBBB) is having an acute myocardial infarction (AMI)?
At the end of the day: How do I know if my patient with a left bundle branch block (LBBB) is having an acute myocardial infarction (AMI)?
- Sgarbossa A: Concordant ST segment elevation in any lead = AMI
- Sgarbossa B: Concordant ST segment depression in V1, V2, or V3 = AMI
- Revised Sgarbossa C: Discordant ST segment > 25% size of R or S wave = AMI [pending validation study]
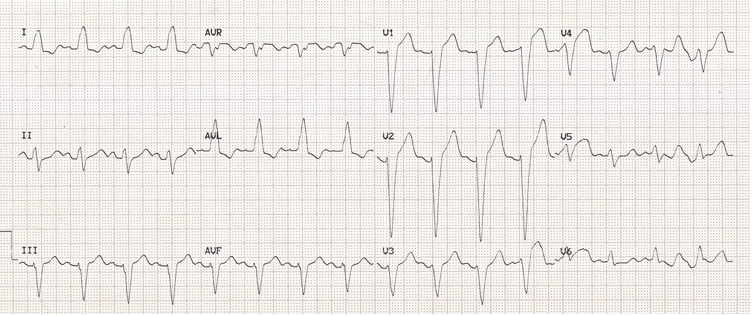
Hold on, what’s a left LBBB? A powerful leftward force; on ECG you should see several criteria:
Tintinalli:
- Prolonged QRS duration (>0.12 s)
- Small R wave followed by deep S wave-leads II, III, aVF, and V1-V3.
- Large and wide R waves-leads 1, aVL, V5 and V6.
- No Q waves in leads 1, V5, and V6.
Tintinalli, however, does not mention that there should also be:
- Appropriate discordance: When the QRS points up, the ST segment should be a little bit depressed. When the QRS points down, the ST segment should be a little elevated. Recognizing the appropriate discordance is key to not missing an MI. Click below to enlarge.
 A LBBB refresher from Life in the Fast Lane: http://lifeinthefastlane.com/ecg-library/basics/left-bundle-branch-block/
A LBBB refresher from Life in the Fast Lane: http://lifeinthefastlane.com/ecg-library/basics/left-bundle-branch-block/
Relatively recent changes: A new LBBB does not predict high likelihood of AMI (Kontos 2011, Jain 2011, Chang 2009). Thus, in the 2013 American College Cardiology (ACC)/American Heart Association (AHA) STEMI guidelines, a new LBBB (or presumed new) is no longer an indication for cath lab activation or lytics (O’Gara 2013).
So when should my patient with a LBBB go to the cath lab? A patient with cardiopulmonary symptoms + LBBB → cath lab/lytics if:
- Hemodynamically unstable or acute heart failure, OR
- Concordant ST segment changes (Sgarbossa rules A or B), OR
- ST:S ratio ≤ -0.25. In other words, discordant ST deviation ≥ 25% of the size of R or S (Smith 2012, Cai 2013). [needs validation]
- Sgarbossa A: Concordant ST elevation ≥ 1mm in any lead = AMI
- Sgarbossa B: Concordant ST depression ≥ 1mm in V1, V2, or V3 = AMI
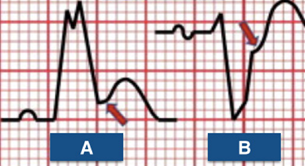
- Revised Sgarbossa C: Discordant ST deviation ≥ 25% of the size of R or S = AMI. (Pending validation)
 More from Dr. Smith, lead author of modified Sgarbossa: http://hqmeded-ecg.blogspot.com/2012/09/modified-sgarbossa-rule-published_4.html
More from Dr. Smith, lead author of modified Sgarbossa: http://hqmeded-ecg.blogspot.com/2012/09/modified-sgarbossa-rule-published_4.html
 To paraphrase Mattu, you can replace the 3rd step (Sgarbossa score ≥ 3) with Sgarbossa A or B. In other words, in place of using the score, if Sgarbossa A -> Primary PCI or lytics; or if Sgarbossa B -> Primary PCI or lytics. If neither, move on to looking for revised Sgarbossa C (T:S ratio ≤ -0.25, i.e. , discordant ST deviation ≥ 25% of the size of R or S (Smith 2012, Cai 2013). [needs validation]
To paraphrase Mattu, you can replace the 3rd step (Sgarbossa score ≥ 3) with Sgarbossa A or B. In other words, in place of using the score, if Sgarbossa A -> Primary PCI or lytics; or if Sgarbossa B -> Primary PCI or lytics. If neither, move on to looking for revised Sgarbossa C (T:S ratio ≤ -0.25, i.e. , discordant ST deviation ≥ 25% of the size of R or S (Smith 2012, Cai 2013). [needs validation]
Amal Mattu’s Sgarbossa Case:
References:
Largely adapted from Amal Mattu’s EKG weekly June 1, 2015
Cai Q, Mehta N, Sgarbossa EB, et al. The left bundle-branch block puzzle in the 2013 ST-elevation myocardial infarction guideline: From falsely declaring emergency to denying reperfusion in a high-risk population. Are the Sgarbossa Criteria ready for prime time? American Heart Journal. 2013;166(3):409–413.
Chang AM, Shofer FS, Tabas JA, et al. Lack of association between left bundle-branch block and acute myocardial infarction in symptomatic ED patients. Am J Emerg Med 2009;27(8):916–21.
Jain S, Ting HT, Bell M, et al. Utility of left bundle branch block as a diagnostic criterion for acute myocardial infarction. Am J Cardiol 2011;107(8):1111–6.
Kontos MC, Aziz HA, Chau VQ, et al. Outcomes in patients with chronicity of left bundle-branch block with possible acute myocardial infarction. American Heart Journal 2011;161(4):698–704.
Neeland IJ, Kontos MC, de Lemos JA. Evolving considerations in the management of patients with left bundle branch block and suspected myocardial infarction. J Am Coll Cardiol 2012;60(2):96–105.
O’Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction. JAC 2013;61(4):e78–e140.
Piktel, Joseph S. (2011). Tintinalli’s Emergency Medicine, A Comprehensive Study Guide. (7th Ed.). New York, NY: McGraw Hill.
Smith SW, Dodd KW, Henry TD, et al. Diagnosis of ST-Elevation Myocardial Infarction in the Presence of Left Bundle Branch Block With the ST-Elevation to S-Wave Ratio in a Modified Sgarbossa Rule. Ann Emerg Med. 2012;60(6):766–776.
