HPI
- 72 yo M with PMH HTN BIBEMS for L sided back pain
- Started after eating
- Denied antecedent vomiting
- Pain associated with dyspnea
Abd: Soft, NT
STUDIES
EKG: NSR, no TWIs or ST deviations
POCUS: Possible L-sided pneumothorax
Labs: Unremarkable
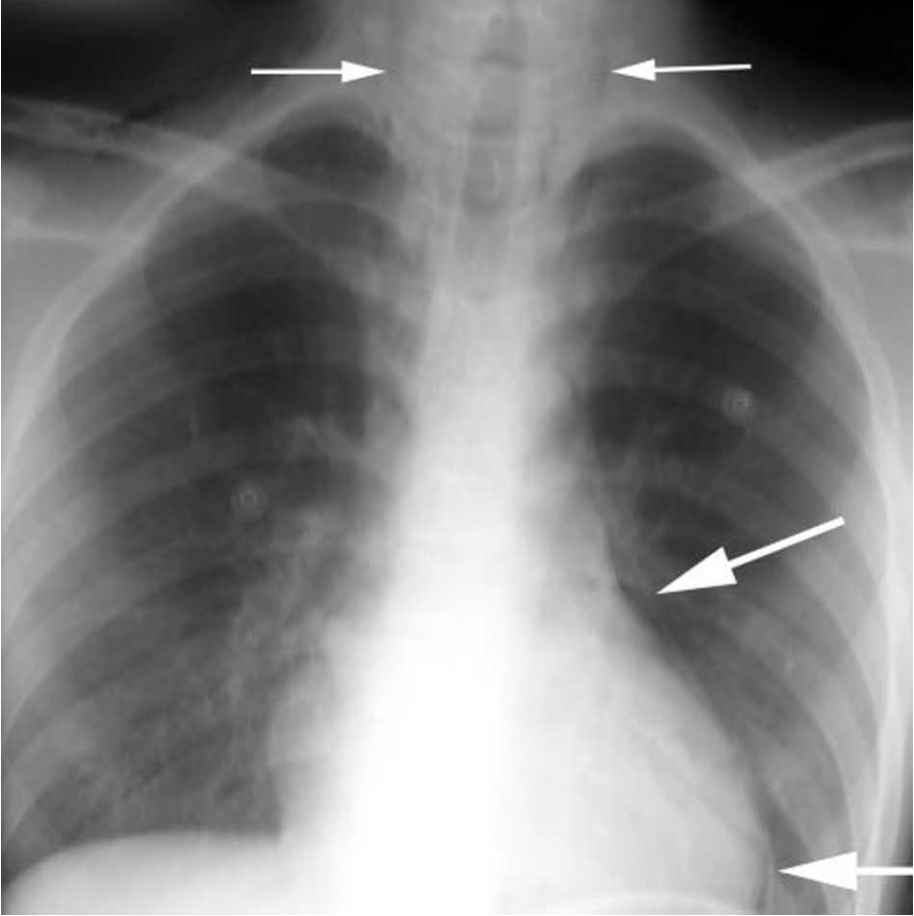
CXR: L-sided hydropneumothorax, pneumomediastinum
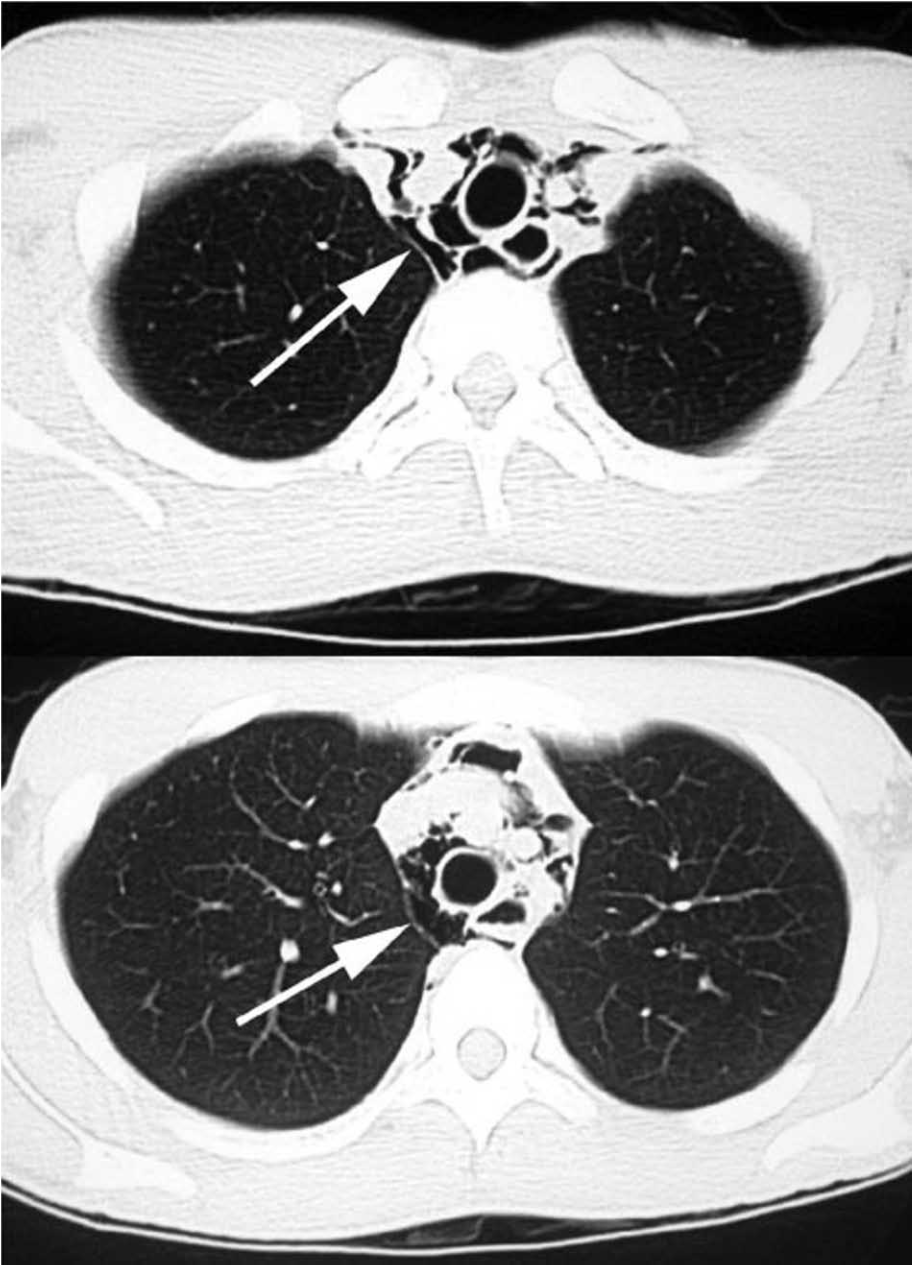
CT Thorax: Boerhaave syndrome with L-sided pneumothorax, extensive pneumomediastinum
- From sudden increase in esophageal pressure/decrease in intrathoracic pressure
- Vomiting
- Childbirth
- Seizure
- Prolonged coughing/laughing
- Weightlifting
- 15% of esophageal perforations
- Most iatrogenic > FB or malignancy
- Most common location of perforation: L posterolateral aspect of distal intrathoracic esophagus
- Gastric contents in mediastinal cavity → chemical mediastinitis → bacterial infection
- Pleural cavity may be violated from inflammation or initial perforation
- ~100% mortality if untreated
- Symptoms (% of pts)
- Chest pain (89%)
- Dyspnea (67%)
- Dysphagia (3%)
- Neck pain (11%)
- Neck swelling (6%)
- Hoarse voice (6%)
- History of retching (NB: 25-45% don’t have history of vomiting)
- Crepitus with palpation of chest wall
- Hamman’s sign: mediastinal crackling with heartbeat
- Within hours:
- Odynophagia, dyspnea, mediastinitis, sepsis
- CXR
- Not sensitive; may require hours for signs to develop
- Findings
- Mediastinal/free peritoneal air/SQ emphysema
- Pleural effusion
- Mediastinal widening
- CT
- Findings
- Esophageal wall edema/thickening
- Mediastinal widening
- Air/fluid in pleural spaces/retroperitoneum
- Findings
- NPO
- Broad spectrum abx
- Protonix gtt
- CT Surgery consult
- Surgical candidates:
- Diffuse extravasation
- Extension of perforation
- Sepsis
- Progression of pneumomediastinum or pneumothorax
- Patients with empyema
- Surgical candidates:
REFERENCES
Blencowe NS, Strong S, Hollowood AD. Spontaneous oesophageal rupture. BMJ 2013;346:f3095.
Carrott PW, Jr., Low DE. Advances in the management of esophageal perforation. Thorac Surg Clin 2011;21:541-55.
Henderson JA, Peloquin AJ. Boerhaave revisited: spontaneous esophageal perforation as a diagnostic masquerader. Am J Med 1989;86:559-67.
Newcomb AE, Clarke CP. Spontaneous pneumomediastinum: a benign curiosity or a significant problem? Chest 2005;128:3298-302.
Triadafilopoulos G. “Boerhaave syndrome: Effort rupture of the esophagus.” Up To Date. http://www.uptodate.com, 26 Apr. 2016. Web. 28 Nov. 2016. https://www.uptodate.com/contents/boerhaave-syndrome-effort-rupture-of-the-esophagus
