ECG of the Block
11/25/2015
Article Inspired by: Dr. Lauren Williams
THE CASE
CC: ‘I just don’t feel well’
HPI:
- 72 yo F PMH ESRD on HD
- c/o weakness and malaise
- Near collapse but denies LOC
- Denies palpitations, SOB, CP, HA, N/V, dysuria, abdominal pain, melena or hematochezia
- Due for scheduled dialysis on day of presentation
Physical Exam
VSS
General: AAOx3, NAD
HEENT: MMM
CVS: RRR, S1, S2, holosystolic murmur
Pulm: CTAB
Abd: Soft, NT
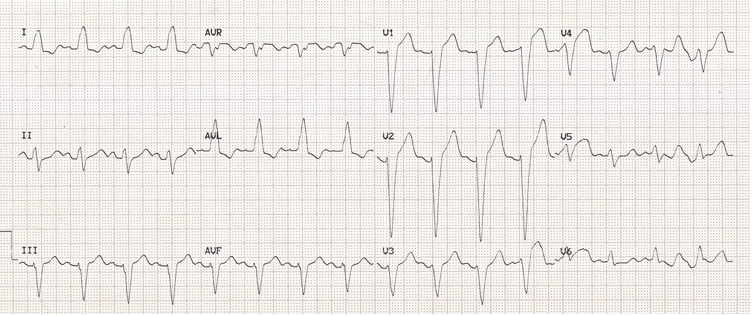
EKG not done at triage but performed at your request after evaluating patient:

THE TALK
Definitions
- Hyperkalemia = potassium level > 5.5 mEq/L (a/w repolarization abnormalities)
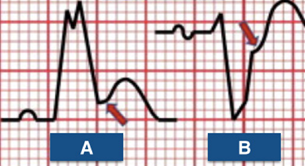
- Peaked T waves
- Moderate hyperkalemia = serum potassium > 6.0 mEq/L (a/w progressive paralysis of the atria)
- P wave widening/flattening
- PR segment prolongation
- Eventual disappearance of P waves
- Severe hyperkalemia = serum potassium > 7.0 mEq/L (a/w conduction abnormalities and bradycardia)
- Prolonged/bizarre QRS morphology
- High-grade AV block with slow junctional or ventricular escape rhythms
- Conduction blocks
- Sinus bradycardia/slow AF
- Eventual development of a sine wave appearance
- Serum potassium level of > 9.0 mEq/L can cause cardiac arrest
- Asystole
- Ventricular fibrillation
- PEA with a bizarre, wide complex rhythm
- In individual patients, serum potassium level may NOT always correlate with the EKG changes
How do I treat hyperkalemia?
- First step: Antagonize the cardiac membrane effects of potassium (with calcium)
- Hypocalcemia can increase the cardiotoxicity of hyperkalemia
- Effect of calcium begins within a few minutes and lasts for ~30-60 minutes
- Indicated only when patient has EKG changes
- Should be administered as infusion given short half-life
- Second step: Drive the extracellular potassium into the cells (insulin with glucose, sodium bicarbonate, and beta-2 adrenergic agonists)
- Insulin enhances the activity of the sodium-potassium-ATPase pump in skeletal muscle
- Effects begins w/in 10-20 minutes, peaks at 30-60 minutes and last for 4-6 hours
- Glucose is usually given with insulin to prevent hypoglycemia
- Beta-2-adrenergic agonists (ex: albuterol)- similar to insulin
- Beta-2-adrenergic receptors in skeletal muscle also activate the inwardly directed Na-K-2Cl cotransporter
- Additive effect when used with insulin and glucose.
- Sodium bicarbonate raises serum pH, resulting in hydrogen ion release from the cells -> accompanying potassium movement into the cells
- Insulin enhances the activity of the sodium-potassium-ATPase pump in skeletal muscle
- Third step: Remove potassium from the body
- Loop/thiazide diuretics
- Limited data to support their use but makes sense clinically to give them if pt not in renal failure
- Cation exchange resin
- A/w intestinal necrosis even after one dose (esp in post-op patients, those with ileus, or bowel obstruction)
- Should only be considered in patients with severe hyperkalemia and ESRD when dialysis is not available
- Dialysis
- Loop/thiazide diuretics
- In a hemodialysis patient, treating hyperkalemia acutely with these medications could drive potassium into the cells, which could then diminish subsequent potassium removal during the dialysis session if performed right afterwards, leading to rebound hyperkalemia after dialysis
TAKE HOME POINT: If a triage ECG is not done for your dialysis patient, that 10 second strip of paper should be at the top of your priority list.
REFERENCES
Williams L. “EKG of the block: Hyperkalemia” Jacobi Medical Center. Jacobi/Montefiore Emergency Medicine Conference. Bronx. November 2015. Case presentation
“ECG Features of Hyperkalaemia.” Burns, Edward. Life in the Fast Lane Medical Blog. LITFL, Web.
“Treatment and Prevention of Hyperkalemia in Adults.” Mount, David. UpToDate, Web.